

Top>Research>Development of a Motorized Glove for Supporting the Functional Recovery Training of Stroke Patients
 Index
Index

Shunji Moromugi [profile]
Development of a Motorized Glove for Supporting the Functional Recovery Training of Stroke Patients
Shunji Moromugi
Associate Professor, Faculty of Science and Engineering, Chuo University
Areas of Specialization: Biometric Information Measurement, Medical Technology & Welfare Engineering
A stroke causes necrosis of brain cells due to clogging or rupturing of blood vessels in the brain. It is estimated that about 300 thousand people suffer a stroke every year in Japan. Even if appropriate treatment is received upon occurrence and a dangerous condition is avoided, there are many cases of aftereffects including motor paralysis in the arms and legs. Recovery from such symptoms requires long-term rehabilitation.
During rehabilitation of the upper limbs after a stroke, special emphasis is placed on functional recovery of the fingers. This is because recovery of finger functions will increase the frequency for hand usage in daily life. It also enables the usage of diverse rehabilitation programs at medical institutions such as rehabilitation clinics, thus leading to early functional recovery for all of the upper limbs. However, the majority of finger rehabilitation training conducted at medical institutions consists of finger exercises conducted by the bare hands of a physical therapist or upper limb training using a peg board. Such training essentially requires constant one-to-one care attention. This often makes it difficult to conduct sufficient rehabilitation at hospitals with many patients. In view of the declining birth rate and aging population in Japan, there is a need for a rehabilitation method which can be implemented more effectively by fewer staff members.
Based on these conditions, my laboratory is developing a motorized glove system for stroke patients, in joint cooperation with Professor Toshio Higashi at the Nagasaki University Graduate School of Biomedical Sciences. Despite featuring a compact and lightweight configuration, this glove system will enable complex finger exercises similar to those performed by physical therapists. In this article, I would like to introduce the system being developed, as well as the results of recent clinical testing.
System overview

Fig 1: Prototype system
The glove system under development can be divided into three main components: (1) a glove worn on the user’s hand, (2) a controller which regulates movement of the glove, and (3) a muscle activity sensor which reads the intentions of the user. Figure 1 shows a photograph of the prototype glove system. Shown in the upper half of the photograph is the case which contains the controller. Specifically, the case contains the drive unit, the microcomputer control circuit, and the sensor signal processing circuit. The sensor and glove can be stored inside the lid of the case, making it possible to carry the entire system in a single case. Shown in the middle of the photograph starting from the left, are the muscle activity sensor, the microcomputer control circuit, and the sensor signal processing circuit, with the latter two shown after being removed from the case. The bottom image in the photograph shows the glove portion. The muscle activity sensor is secured to the user’s forearm using an elastic belt. The sensor detects minute amounts of muscular activity which govern extension and flexion movement of the fingers. Using the detected data, the controller can infer the finger movement intended by the user. The glove is made from specially designed leather, the inside of which is laid out resin threads (drive threads) positioned to replicate the tendons of a human hand. There are a total of four threads, two of which support extension of the fingers and two of which support flexion of the fingers. The drive threads are connected to the drive unit of the controller. Based on the user’s intended finger movement as detected by the sensor, the controller changes the shape of the glove by pulling individual threads via the power transmission cable. This realizes finger movement that accompanies a variety of finger movement paths. The prototype system shown here is for experimental use only and is therefore designed to enable movement of either the pointer finger or middle finger.
Possible finger rehabilitation training
Finger rehabilitation training using the glove system is implemented in the following order. First, the glove is put on the user’s fingers. Next, using the manual operation mode of the system, the doctor or physical therapist operates the compact lever of the microcomputer control circuit in order to change the finger position of the patient wearing the glove. At the same time, the operator pushes the button in order to save multiple finger positions in the controller. After saving the finger positions, pressing the start button will cause the controller to change the glove into the recorded finger positions in sequential order while conducting interpolation. As a result, finger movement is performed following the finger movement paths intended by the doctor or physical therapist. The finger movement is only conducted when the user is making an effort to straighten or bend his/her fingers. When the user relaxes, finger movement stops. It is also possible to input a specified number of times for finger movement into the controller in advance. For example, if the physician saves a movement like tracing a circle with the fingertip, sets the number of times to 100 and presses the start button, it is possible to perform 100 sets of fingertip circular movement training with movement effort from the user.
Clinical tests

Fig 2: Scene of clinical testing
Through cooperation from Miharadai Hospital in Nagasaki City, we performed tests to verify the efficacy of finger rehabilitation training using the glove system. The test subject was a 87-year old female who had suffered a stroke seven years ago. Since then, the subject suffered from right hemiplegia and had difficult grasping objects with her right hand. For only a 25-day period (intervention period) during daily upper limb rehabilitation training at the hospital, the system was used to perform an additional 20 minutes of fingertip circular movement training. A scene from rehabilitation training using the glove system is shown in Figure 2. In order to assess upper limb movement function, we used the Simple Test for Evaluating Hand Function (STEF), the Hemiparesis 10-Second Test, and the Motor Activity Log-Amount of Use (MAL-AOU) Test. All of these tests are widely used in the evaluation of upper limb movement function in stroke patients. Due to length limitations of this article, I will omit an explanation of test details.
The tests used AB design in single case study. In other words, a 15-day period (A) prior to intervention was established as the baseline. Then, scores for each test were compared with a 25-day period (B) after intervention. During a total 40-day period, upper limb function was evaluated every five days. Measurement data was obtained for a total of eight times: three times prior to intervention and five times during the intervention period. Data analysis was performed based on 2-standard deviation (SD) band analysis. In this analysis method, interpretation is based on graph readings instead of statistical methods. Rehabilitation was judged as effective if the score during intervention was higher than the average score (baseline) prior to rehabilitation intervention plus two times the standard deviation for that period.
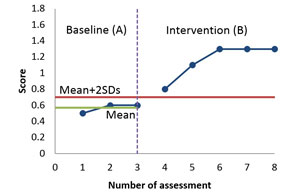
Fig 3: Motor Activity Log-Amount of Use (MAL-AOU) during test period
All test scores show an increase during the intervention period when compared to the baseline period. Although testing was conducted for a single subject only, we confirmed outstanding results in finger movement rehabilitation when using the glove system. Figure 3 shows measurement results for the MAL-AOU Test. This data shows that functioning of fingers on the paralyzed side improved after beginning rehabilitation using the glove system. A significant increase in the frequency of use during daily life can also be observed.
The results of our research were presented last year at the International Conference on NeuroRehabilitation (ICNR 2014), an event which is related to cranial nerve engineering and was held in Aalborg City, Denmark.
Toward a new training method to enable early functional recovery
For people suffering from aftereffects of a stroke like motor paralysis, achieving functional recovery to the greatest possible extent and returning to a normal lifestyle are urgent issues. Our research proposes a lightweight and compact motorized glove as a new method for functional recovery training, and the glove is under development. The glove system mainly targets patients who suffer from upper limb paralysis as the result of a stroke. Currently, a prototype system has been used to perform clinical testing on a single subject. Results showed a certain extent of results. In the future, we shall conduct tests on even more subjects in order to obtain a more detailed assessment of results. We shall also continue to refine the glove system in order to realize even more effective upper limb rehabilitation.
Reference Literature
- (1) Koji Shomoto; Importance of Single Case Design – Physicotherapeutics, Volume 34-4, pp 202 to 205 (2007)
- (2) S. Moromugi, T. Higashi, R. Ishikawa, S. Kudo, N. Iso, S. Ooso, T. Shirotani, M. J. Lawn, T. Ishimatsu, Exotendon glove system for finger rehabilitation after stroke, Replace, Repair, Restore, Relieve – Bridging Clinical and Engineering Solutions in Neurorehabilitation, Biosystems & Biorobotics, Volume 7, 2014, pp 93 to 102 (2014)
-
Shunji Moromugi
Associate Professor, Faculty of Science and Engineering, Chuo University
Areas of Specialization: Biometric Information Measurement, Medical Technology & Welfare Engineering - Shunji Moromugi was born in Kagoshima Prefecture in 1973. He graduated from the Program of Mechanical System Engineering in the School of Engineering, Nagasaki University in 1997.
He completed the Master’s Program in the Graduate School of Information Systems, The University of Electro-Communications in 1999.
He completed the Doctoral Program in the Henry Samueli Graduate School of Engineering, University of California, Irvine in 2003. He holds a Ph.D. from UC Irvine.
He was appointed as Research Associate in the School of Engineering, Nagasaki University in 2002. He was appointed as Assistant Professor in the School of Engineering, Nagasaki University in 2007.
He has been appointed as Associate Professor in the Department of Electrical, Electronic and Communication Engineering in the Faculty of Science and Engineering, Chuo University since April, 2014.
His current research themes include technology to support the disabled through the application of biometric information measurement technology and robot technology, as well as the development of medical robots and medical devices.

- Research Activities as a Member of Research Fellowship for Young Scientists (DC1), Japan Society for the Promotion of Science (JSPS) Shuma Tsurumi
- Important Factors for Innovation in Payment Services Nobuhiko Sugiura
- Beyond the Concepts of Fellow Citizens and Foreigners— To Achieve SDGs Goal 10 “Reduce Inequality Within and Among Countries” Rika Lee
- Diary of Struggles in Cambodia Fumie Fukuoka
- How Can We Measure Learning Ability?
—Analysis of a Competency Self-Assessment Questionnaire— Yu Saito / Yoko Neha - The Making of the Movie Kirakira Megane